Otoplasty (Correction of prominent ear)
The dimensions of a normal ear is 6.5 x 3.5 cm. The size of the ear reaches to 85 % of the mature size until the age of 3; and reaches to 90 % until teh age of 6. The distance of the outer rim of the ear is 15-20 mm (Figure 1). If the rim is more distant than these values, it is called prominent ear.
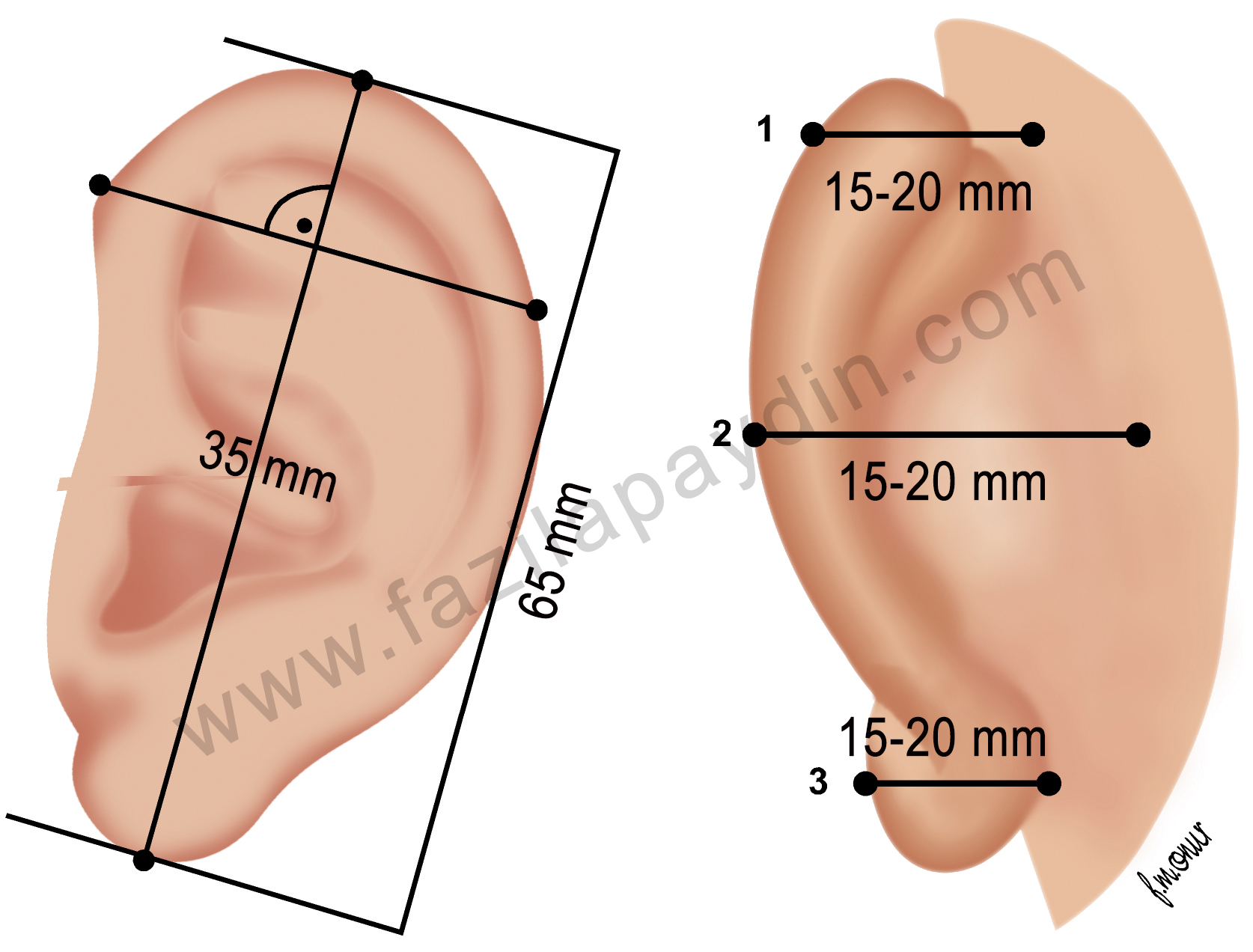
Figure 1: The size of the ear and its distance from the head.
The most frequent problems in prominent ear are: (Figure 2)
- The absence of antihelix,
- Overgrown conchal bowl,
- Prominent lobule,
- Prominent upper pole,
- Irregularities of the helix,

Figure 2: The most frequent problems in the prominent ear are shown in these pictures.
What are the goals of otoplasty?
- The prominent upper pole must be corrected
- In frontal view, the helix and antihelix should both be seen
- The outer rim (helix) should be smooth
- The posterior groove of the ear touching the head should be preserved
- The distance of the helix from the head should be 15-20 mm
- The difference in ear-head distance among both ears should not exceed more than 3 mm.
When should the operation been done?
This deformity can cause some psychological disturbances among children when they start elementary school. That is why it is usually aimed to make the operation before the child starts school. It should be remembered that the size of the ear reaches almost to adult size at the age of 6. By doing so, the ridicule in the school can be prevented.
What kind of anesthesia is needed?
In children, the operation is performed under general anesthesia. In adults it can be done under local anesthesia.
How is the surgery done?
The operation starts with an incision behind the ear to expose the posterior surface of the deformed cartilages. There are mainly three methods to create antihelix (Figure 3):
- Cartilage cuts and sutures (Converse)
- Cartilage scoring (Stenström)
- Sutures (Mustardé)
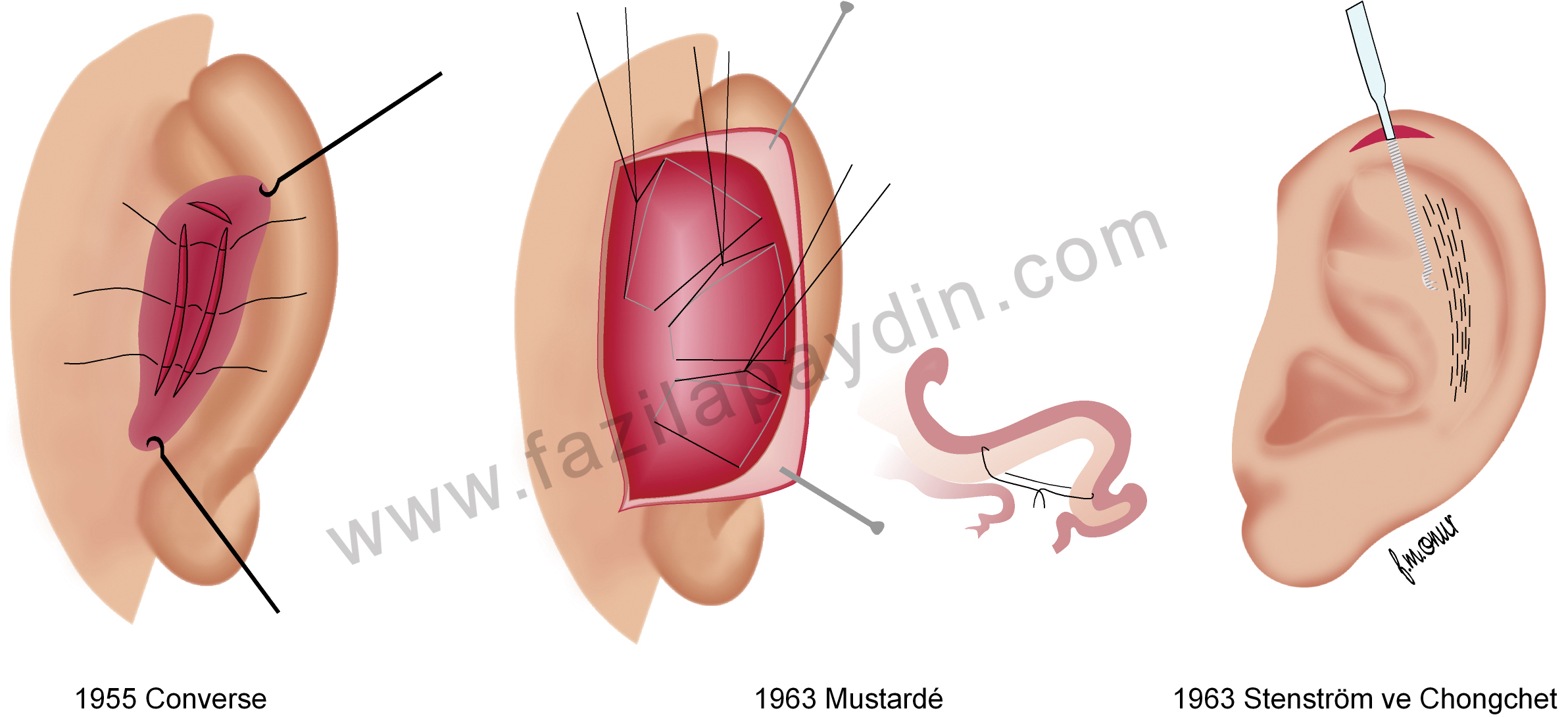
Figure 3: Three methods to create antihelix.
Moreover, if the conchal bowl is too big or distant from the mastoid bone, cartilage can be resected or sutured to the bony surface after removing soft tissues (Figure 4). Then the ears are wrapped up by gentle bandages to apply slight pressure on the ears.
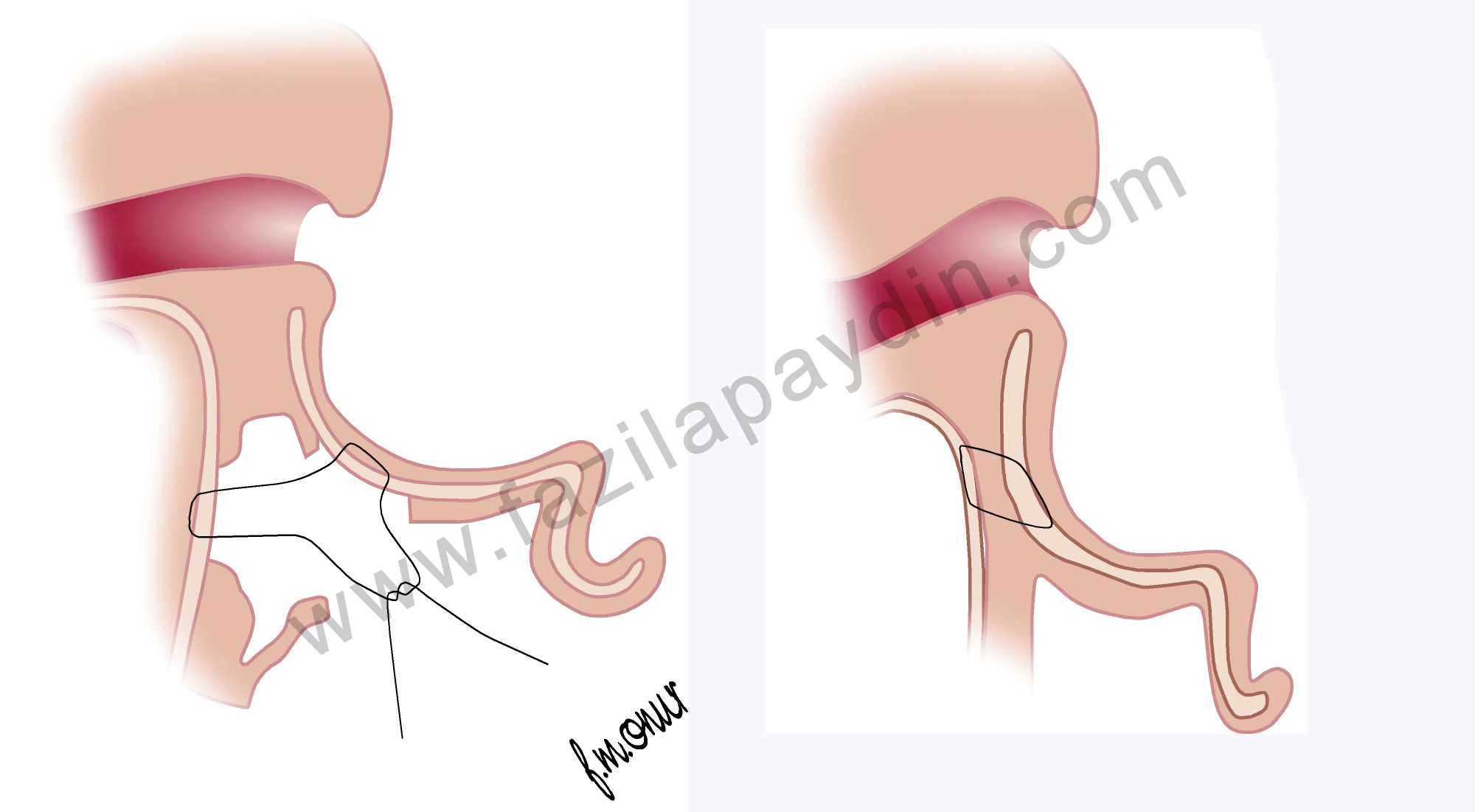
Figure 4: Conchal bowl can be approximated to the head by sutures.
Are the skin incisions always placed in the posterior surface of the ear?
The answer is simply No. Because some surgeons prefer to use the anterior approach and keep the posterior ear groove intact. In certain situations, I sometimes use this technique as well (Figure 5).
Her zaman kulak arkasından kesi ile mi ameliyat yapılmaktadır?
Kulak arkasında kesi yapmanın mümkün olmadığı bazı durumlarda, kulak arkası çukurunun original olarak korunması gereken durumlarda iyi bir alternatif de kulak ön kısmından çukur kıkırdağın üs kısmından kesi ile girmektir. Bu sayede büyük çukur kıkırdak küçültülürken aynı zamanda iç çerçeve de oluşturulabilir (Şekil 5).
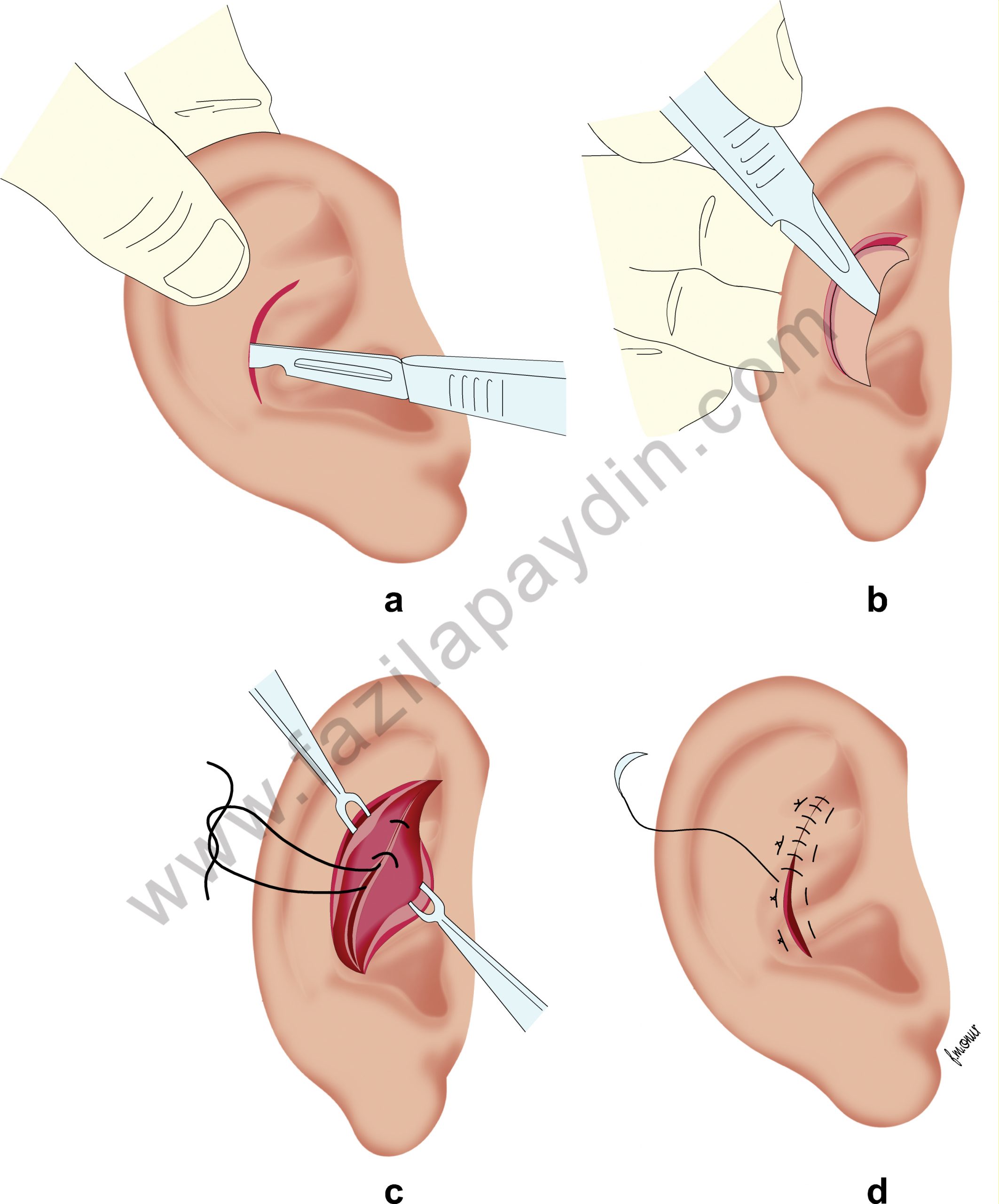
Figure 5: Through an anterior approach, conchal excess cartilage can be resected as well.
Is it possible to do this operation without sutures?
Yes. It has been described and used for decades. In mild and selected cases, it can be done.
Do you apply any dressing or bandage after surgery?
The dressing applied after surgery is changed one day after surgery and repeated every other day afterwards. The head is kept wrapped up for a week. Then the patient is asked to apply a bandana type bandage on the ears while sleeping for an additional week.
Is there any risk of complications?
As in all surgical procedures, in otoplasy there are some risks, but very minor indeed.
Complications (General)
- Bleeding
- Infection
- Cartilage infection
- Numbness
- Temporary facial paralysis due to local anesthetic injection
- Keloid (Hypertropied wound healing)
- Skin loss
- Suture reaction
- The obliteration of the posterior ear groove
Complications (Aesthetic)
- Asymmetry or inadequate correction (most often seen complication)
- Overcorrection
- Reappearance of the prominent ear
- Telephone ear deformity
- Narrowing of the external auditory canal



